Chronic wound treatment: 5 patient success stories
Discover faster healing with an advanced wound dressing.
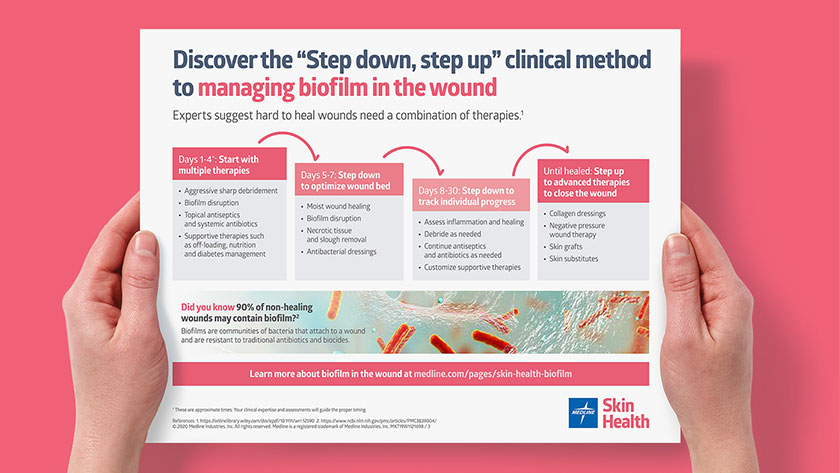
You strive to provide the best possible wound care, but patients with chronic wounds present complex challenges. Experts now agree that biofilm may be the cause of a stalled wound healing process. More than 90% of chronic wounds and some acute wounds may contain biofilm.1 Wounds such as venous leg ulcers, diabetic foot ulcers and pressure injuries may all contain biofilm.
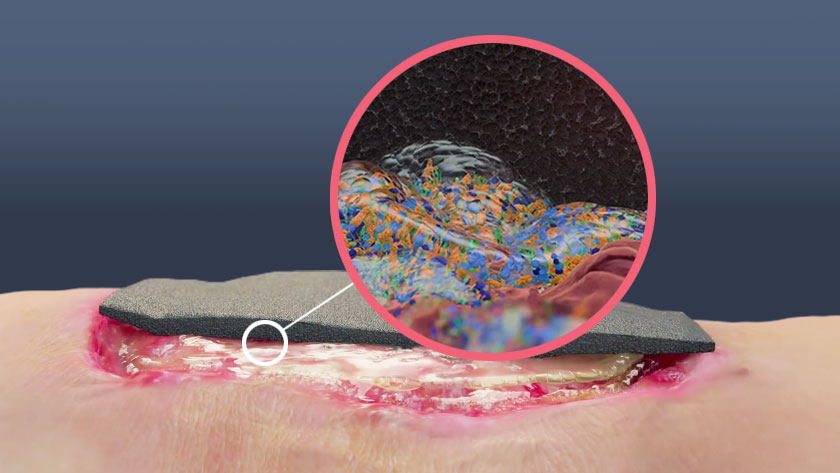
Biofilm in the wound
Biofilm is a community of bacteria that’s encased in a protective environment, making it more difficult for traditional therapies to work. That’s why it’s important to have the most advanced wound care products available to help promote wound healing.
There are many choices for dressings for chronic wounds, but the innovative technology of PluroGel Burn and Wound Dressing uses surfactant micelles to hydrate the wound, control exudate and support autolytic debridement. It softens, loosens and traps debris to de-slough the wound bed, and helps remove necrotic tissue due to its surfactancy effect of the extracellular matrix. It has also been shown in vitro to both disrupt biofilm and prevent it from rebuilding based off in in vitro testing.2
The science behind PluroGel. Watch video
Below are five case studies that demonstrate the power of PluroGel as a therapy for managing chronic wounds in a timely manner.
Surfactant-based wound gel helps reduce wound size and lower patient reported pain3

Patient: 70-year-old male
Wound: Long-standing wound on lower leg that had considerable exudate, foul odor, and a painful, friable, dark-red wound bed, which made it difficult to cleanse and debride; patient-reported pain level of 8 out of 10.
Initial treatment: Antibiotics, as well as multiple dressing types at various times, including silver and methylene blue and gentian violet.
Change in therapy: Other wound dressings were replaced with PluroGel, a silicone foam dressing and compression therapy. The wound was cleansed with saline and the dressing was changed daily.
Results: After eight weeks, the wound size had shrunk from 39.70cm2 to 7.35cm2, with the patient reporting no pain during or after dressing changes.
Wound deemed “not healable” improves with PluroGel3

Patient: 85-year-old man
Wound: Large wound on the lower limb that was 22.04cm2 with a wound bed described as friable, slightly malodorous and tender when touched. It had a moderate amount of exudate and some periwound maceration.
Initial treatment: The patient’s wife cared for him with a prescribed two-layer light compression system and saline cleansing. In-home clinicians tried various dressing products including a variety of silver, but the wound failed to respond, and they concluded it was “not healable.”
Change in therapy: PluroGel with light compression.
Results: After five days, the wound had reduced to 15.60cm2 and showed healthy granulation tissue. At seven weeks, it was down to 7.70cm2 and, by six months, the wound was considered fully healed. Previously, the recalcitrant wound had a negative effect on the patient’s health-related quality of life, as well as the wife’s, who felt responsible for the condition of the wound.
After multiple therapies, PluroGel showed better results4

Patient: 29-year-old male
Wound: Wound on lower leg (wound on right in image), almost completely covered in dark green, moist, devitalized tissue.
Initial treatment: Sometimes compression stockings or socks, and a variety of wound dressings depending on exudate, bioburden and pain levels.
Change in therapy: To determine the best therapy, PluroGel was applied to the wound on the right. The patient changed the dressing daily.
Results: When the patient returned to the wound clinic after six days, the PluroGel-treated wound showed a 95% reduction in devitalized tissue, as well as evidence of granulation tissue forming.
One week to improve sacral pressure injury5

Patient: 75-year-old with history of incomplete L1 paraplegia, incontinence and other chronic medical issues.
Wound: Sacral pressure injury covered in slough with an island of eschar.
Therapy: Application of PluroGel, along with other pressure injury prevention measures.
Results: After seven days, the eschar had softened and the wound showed beginnings of visible granulation tissue.
Key takeaway
Biofilm may be a key factor in non-healing wounds, and it’s important to arm yourself with all the tools possible to kick-start the healing process. In many real-life cases of chronic wounds, PluroGel Burn and Wound Dressing has been shown to make a significant impact on helping these wounds to shrink and become less painful.
References:
- Attinger C and Wolcott R. Clinically addressing biofilm in chronic wounds. Advances in Wound Care. 2012;1(3):127-132. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3839004/. Accessed September 16, 2019.
- Yang Q, Larose C, Porta AD, Della Porta AC, Schultz GS, Gibson DJ. A surfactant-based wound dressing can reduce bacterial biofilms in a porcine skin explant model. Int Wound J. 2016
- https://doi.org/10.12968/jowc.2018.27.10.664, courtesy Rosemary Hill BSN, CWOCN, WOCC (C), VCH-Coastal-Lions Gate Hospital
- https://doi.org/10.12968/jowc.2018.27.10.664, courtesy Dot Weir, RN, CWON, CWS, Clinical Staff, Saratoga Hospital Center for Wound Healing and Hyperbaric Medicine, Saratoga Springs, NY
- Hill, R., BSN CWOCN CETN(C) & Vancouver Coastal Health-Lions Gate Hospital. (n.d.). Need a biofilm disrupter? Consider application of a concentrated surfactant technology: A case series.
- Ratliff, C. R. (2018). Management of a Groin Wound Using a Concentrated Surfactant-Based Gel Dressing. Journal of Wound Ostomy and Continence Nursing. https://doi.org/10.1097/won.0000000000000467